Pathogenesis Of Rheumatic Fever
The exact mechanism of GAS pharyngitis causing RF is still unexplained. It may be an exaggerated autoimmune response of the host to GAS pharyngitis. The clinical manifestation and severity of RF/RHD in an individual depends on the virulence of the infecting organism, host susceptibility, and environmental factors (Figure 1).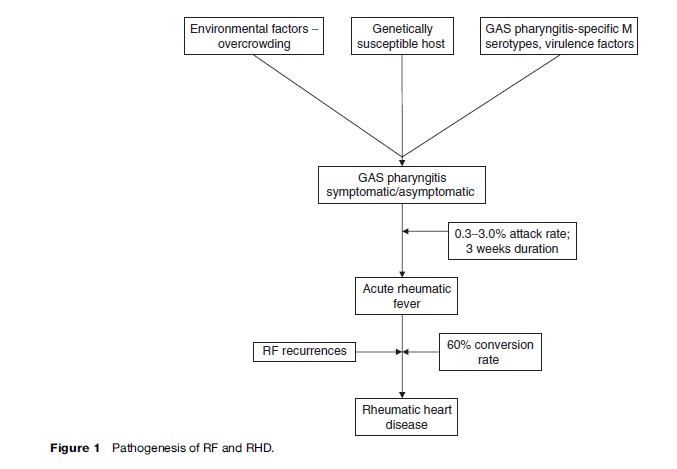
The Organism (Group A Streptococcus Pyogenes)
Among the GAS, not all strains cause RF; it is believed that there are only a few virulent strains with rheumatogenic potential. The specific strains are usually heavily encapsulated and form large mucoid colonies rich in M-protein, which enhances the GAS ability to adhere to tissue and resist phagocytosis. The streptococcal M protein shares the homology with cardiac myosin and tropomyosin, connective tissue keratin and laminin, and therefore results in autoimmune response against the heart, brain, and joints. Only the 1, 3, 5, 6, 14, 18, 19 and 24 M protein serotypes are associated with RF. The role of other GAS antigens such as streptococcal erythrogenic toxin, streptococcal fibronectin binding protein 1 (sfb1), and streptococcal C5a peptidase (SCPA) have also been demonstrated in the pathogenesis of streptococcal infection.The Host
It is consistently observed that only 0.3–3.0% of individuals with acute GAS pharyngitis develop RF, because of different genetically determined autoimmune responses and susceptibility to infection. Various genetically determined risk factors such as major histocompatible antigens, potential tissue-specific antigens, and antibody and T cell response to streptococcal infection play an important role in the pathogenesis of RF/RHD. Various studies have demonstrated the association of HLA class II alleles with RF/RHD, although the particular alleles are different in different populations: For example, HLA-DR4 is more frequent in Caucasians, HLA-DR2 in African-American populations, HLA-DR1 and DRw6 in South Africa, HLADQW2 in Asians, and HLA-DR3 in India. Association is also being described with high concentrations of mannosebinding lectin and polymorphisms of transforming growth factor-b1 and immunoglobulin genes. A B cell alloantigen D8/17 has also been found to be associated with susceptibility of acute RF (Kemeny et al., 1994). According to observations worldwide, this alloantigen expression is strongly associated with RF. Further investigations are needed before the particular alloantigen can be widely used to identify individuals at risk for RF/RHD.Environmental Factors
The secular trends of RF/RHD over the years in developed and developing countries suggest that environmental factors such as poor living conditions, overcrowding, malnutrition and poor hygiene, and poor health-care access are the significant determinants of the disease burden and distribution. Crowded living conditions contribute to rapid spread and persistence of virulent strains in the community. Seasonal variations in the incidence of RF are more pronounced in temperate than in tropical climates.
Our Advantages
- Quality Work
- Unlimited Revisions
- Affordable Pricing
- 24/7 Support
- Fast Delivery
Order Now